
What It Took to Change How Pediatric Science Gets Done
When the Gabriella Miller Kids First Pediatric Research Program (Kids First) launched, the premise was ambitious. If we could bring together deeply annotated pediatric data across cancer and congenital disorders, make it open and usable, and pair it with the right technology and community, would discovery accelerate in ways that mattered for children and families?
Ten years is long enough to ask an honest question.
The Kids First Capstone Report reflects on that original idea and what the past decade reveals about the answer.
From fragmented data to a shared foundation
When Kids First began, pediatric research data often lived in isolation. Individual labs or institutions worked with small cohorts, limited tools, and little ability to connect findings across diseases or disciplines. For rare conditions, in particular, no single center had sufficient data to address the most pressing questions.
Kids First set out to change that by building an open science infrastructure designed for collaboration from the start. That work is carried out through the Kids First Data Resource Center (Kids First DRC), which designs, develops, and stewards the platforms and tools that make large-scale pediatric data accessible to the research community. The goal was not just to generate more data, but to make it easier for researchers worldwide to find, access, and use it in meaningful ways.
Ten years later, that foundation is firmly in place.

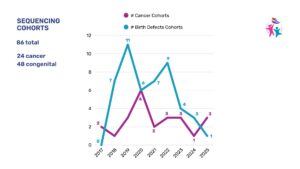
Today, the Kids First Data Resource includes more than 1.56 million data files. Sequencing efforts have supported over 53,000 pediatric patients and more than 9,000 family members, creating one of the most comprehensive pediatric research ecosystems in the world.
This scale did not appear overnight. It was built year by year, through sustained investment, shared standards, and a commitment to doing the hard work of coordination.
When a new way of working becomes the norm
One of the clearest signals of success is when something that once felt novel becomes expected.
 Kids First was designed as a non-local discovery framework. Researchers need not be affiliated with a particular institution, be working on a single disease, or be part of the original data-generating team to contribute. Through the Data Resource Center’s platform architecture and access model, if you have a good question, the infrastructure is there to help you pursue it.
Kids First was designed as a non-local discovery framework. Researchers need not be affiliated with a particular institution, be working on a single disease, or be part of the original data-generating team to contribute. Through the Data Resource Center’s platform architecture and access model, if you have a good question, the infrastructure is there to help you pursue it.
That model has broadened participation in pediatric research. Alongside investigators who generate and curate cohorts, a growing community of secondary users now brings new expertise, methods, and perspectives to the data. Researchers cross disease boundaries, apply tools from one domain to another, and uncover insights that would not surface in siloed systems.
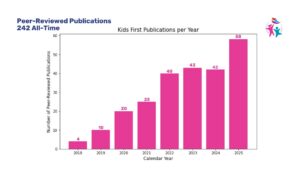
This shift is evident in science. While disease-specific studies remain essential, an increasing share of publications using Kids First data focus on cross-condition and cross-modality analysis. That growth reflects a broader truth. The most powerful discoveries often happen at the intersections.
Data is only valuable if it can be used
Scale alone does not drive impact. Use does.
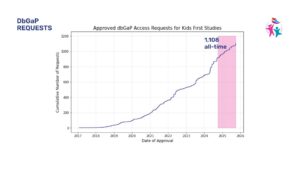 Over the past decade, Kids First has seen steady growth in portal adoption, data access requests, and active compute usage. More than 1,100 data access requests have been approved to date, a strong indicator of trust from the research community. Researchers request access when the data are rigorous, well-curated, and worth the effort.
Over the past decade, Kids First has seen steady growth in portal adoption, data access requests, and active compute usage. More than 1,100 data access requests have been approved to date, a strong indicator of trust from the research community. Researchers request access when the data are rigorous, well-curated, and worth the effort.
Here, Kids First DRC plays a central role, stewarding CAVATICA, a cloud-based analysis environment in which researchers can compute directly on harmonized data. This matters because computing where the data lives reduces friction. When researchers can analyze datasets without moving or duplicating them, discovery accelerates and reproducibility improves.
Across the Capstone findings, the pattern is consistent. When data, tools, and training are aligned, scientific output follows.
Collaboration as an engine for innovation
Kids First was never intended to operate independently.
From the outset, the program was designed to align with broader NIH initiatives and serve as part of a larger ecosystem. The Data Resource Center supports this interoperability by enabling trusted, secure connections between Kids First and other NIH platforms, including the Childhood Cancer Data Initiative, INCLUDE, and other Common Fund programs. Over time, those connections have expanded the reach and relevance of the data.
This interoperability matters because pediatric diseases are complex. Advancing precision medicine requires multimodal data, diverse expertise, and shared infrastructure that can evolve alongside new technologies.
As sequencing, imaging, proteomics, and emerging analytical methods continue to mature, Kids First is positioned to support deeper, more dynamic views of patient data. The long-term vision extends beyond static datasets toward longitudinal, continuously enriched resources that reflect how care and outcomes change over time.
What the first decade teaches us
Looking across ten years of data and experience, several lessons stand out.
Open pediatric data accelerates discovery when it is paired with usable tools and clear pathways to action. Awareness brings researchers in, but usability keeps them engaged.
 Shared infrastructure outperforms fragmented efforts. Researchers consistently prefer to work within systems that reduce duplication, lower costs, and support reproducible science.
Shared infrastructure outperforms fragmented efforts. Researchers consistently prefer to work within systems that reduce duplication, lower costs, and support reproducible science.
Value compounds over time. Each new dataset increases the usefulness of the entire ecosystem, enabling insights that no single study could produce alone.
Perhaps most importantly, collaboration is not a secondary benefit. It is the mechanism through which innovation happens.
Entering the next chapter
The Kids First Capstone Report closes the first decade of the program. The scale achieved in recent years signals a transition to a more mature phase, characterized by integration, expanded participation, and greater impact.
The work ahead will require continued investment, ongoing modernization, and a sustained commitment to openness and equity. It will also need the same community mindset that made the first ten years possible.
Kids First exists because families, researchers, institutions, and federal partners chose to work together toward a shared goal. That collaboration includes the teams that design and operate the Kids First DRC, as well as the broader research community it serves. Together, they have reshaped how pediatric science is done.
As the program enters its second decade, the question is no longer whether this model works. The evidence is clear.
The question now is, how far can it take us next?